



Nurse Files: Amiodarone
Antidysrhythmic


To my annoyance, the brain is not the only organ in the body. It needs other squishy parts like livers and kidneys in order to survive. So, when things go wrong south of the carotids, I need to pay attention.
Not the least of these is the heart. Heart = blood = oxygen = alive brain cells. Therefore, heart = brain cells. I need the heart to continue its cheerful pumping without issue.
Enter: dysrhythmia. There are not too many ways a heart rhythm can go wonky. The intervention of choice depends on whether it’s too fast or too slow, and if it’s organized or not.

Back to Basics:
The heart works due to two coordinating systems:
The electrical signal generated and carried by the cell membranes through the movement of electrolytes.
The strength and coordination of the myocardium reacting to this signal.
If there is something wrong with either of these processes, the heart will not pump efficiently nor effectively. And, as we showed earlier, a working heart means a working brain.
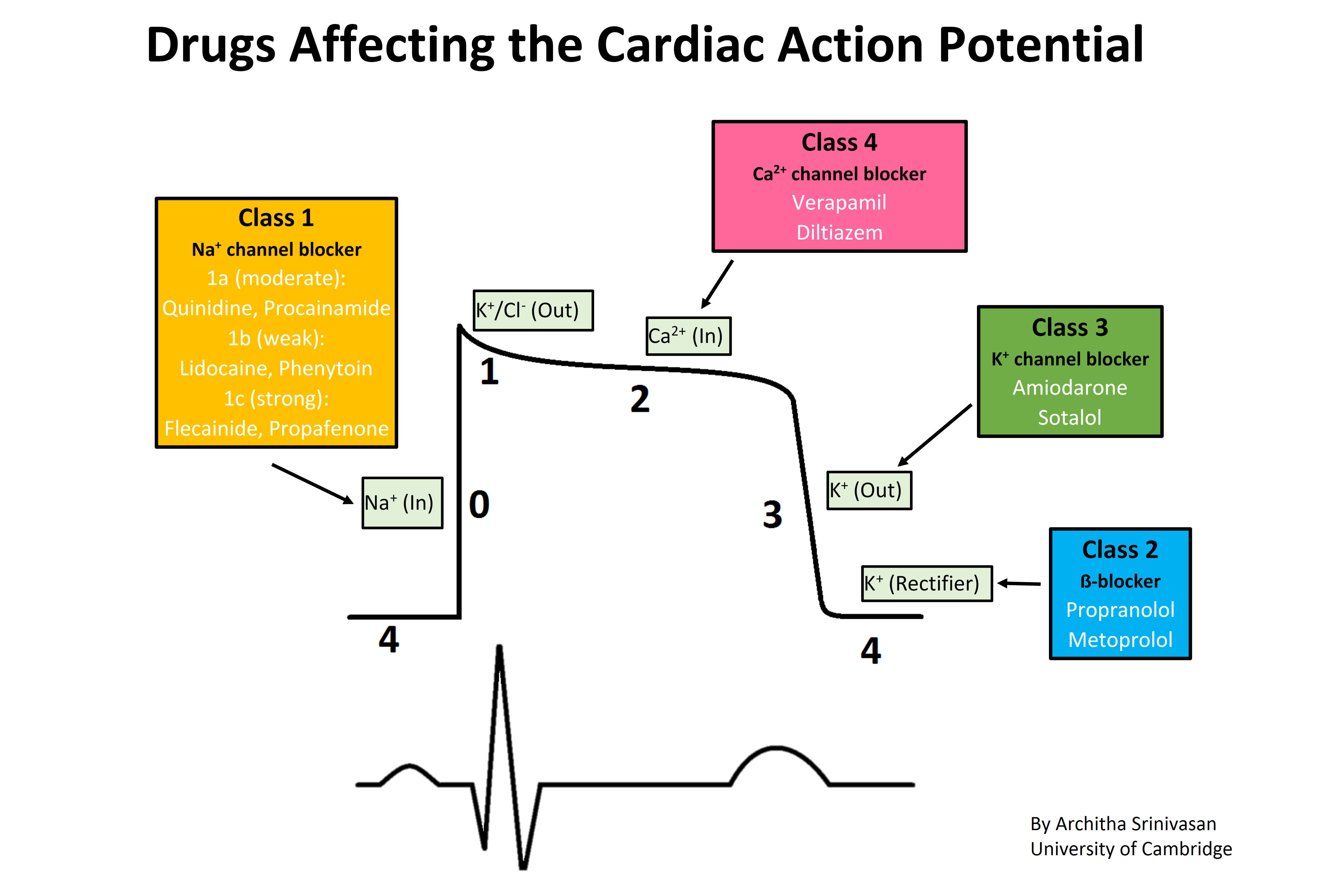
This electrical signal is called the Action Potential, or the AP. (This is also an acronym used in imaging to mean Anterior Posterior, or from the front). The AP relies on the coordinated movement of electrolytes as ions (negatively charged) and cations (positively charged). These move either by active or passive transport across the cell membrane to shift the electrical charge and cause muscular response.
Here is a nice picture of this AP:

The Sinus Rhythm shown with the AP above is what we are aiming for. The atrial and ventricular motion is tidy, everything is working smoothly.
But when it looks something like this:
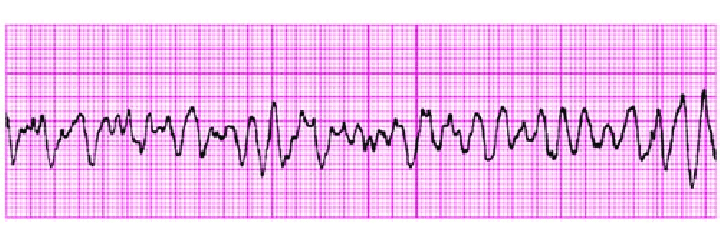
Ew, right? No good for anybody, the patient most of all.
Now, the first step for treating Ventricular Fibrillation (VF) is to start CPR, then shock. Don’t hesitate, don’t ask questions. If the patient is not brushing their teeth and you see the above, call a code and start pumping. Then amiodarone can be used during ACLS to reverse life-threatening dysrhythmia.
In my experience, however, I use amiodarone most to treat Supraventricular Tachycardia (SVT) or Atrial Fibrillation with Rapid Ventricular Response (AF-RVR)(Don't you just love all these acronyms?):
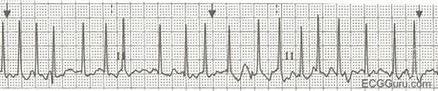
SVT and AF-RVR can look similar due to the speed. Both are disorganized and can lead to cardiogenic shock and ischemia if not treated. Also, bet on your patient’s blood pressure being in the toilet. They probably feel awful, are sweating and clammy, and likely are ready to pass out. Get their feet up, call your doc and/or a Rapid Response, and get this fixed.
How It Works:
If the ECG tracing looks bad, the AP and resulting contractions are just as disorganized. We need to organize it. To do that, we need to calm it the heck down.
Amiodarone is a ‘Class III’ antiarrhythmic drug. The classes are determined by which part of the action potential they target/block.
The mechanism is not fully understood, but amiodarone extends the AP and makes the refractory period longer, thus blocking the myocardium from initiating new APs. No electrical signal = no contractions = no more dysrhythmia.
Bedside Considerations
With all cardioactive meds, there is risk of going too far. If you know your patient has a heart block, this drug is not a good choice. Their AP is already impeded, so we definitely don’t want to make it worse. Also use caution in preexisting heart failure, as the muscle itself may be unable to pump no matter what signals are being sent. Know their history and be ready to give a quick report to the responding team.
Here is my process if I see AF-RVR on my monitor.
Is this something I know they have? Is it new onset or chronic? Is it causing symptoms? If they are crushing candies on their phone in no distress, I probably don’t have to pull out the big guns quite yet.
Assess them. How do they feel? Does their chest hurt? Do a set of vitals. Ask if they’ve had their normal daily medications today. Skipping a few doses of metoprolol with absolutely cause a return of AF.
Ask them to cough. Sometimes a little vasal vagal action will bump things into place. (ICU tip: You can suction a vented patient and get them to cough that way).
If they are symptomatic, i.e., low blood pressure, chest pain, dizziness, alert the medical team and put them on their head. I do not see enough Trendelenburg happening in the hospital. Easiest way to give a patient a 200-300ml bolus is to do a Passive Leg Raise. Their toes don’t need blood if their heart doesn’t have any. This can be tricky in patients with respiratory issues so lay them as flat as possible and slap some Os on their face.
You will probably be instructed to try a metoprolol or diltiazem IV push first. This can tank a blood pressure, but if they have room to wiggle (since you tipped them upside down) this can be very effective. If not, continue on.
Some doctors prefer a diltiazem drip over an amiodarone drip. Both are effective at stopping atrial dysrhythmias, though diltiazem has a greater effect on blood pressure and may not be tolerated (1).
Amiodarone is given as an IV bolus, then a tapered drip over the next 18 or so hours. It is administered through a filtered IV set, as it can cause severe phlebitis.
Be checking vitals at regular intervals, every 5 minutes to start, then every 15 once things calm down. Watch for worsening heart failure by checking skin temperature and moisture, pulses, and respiratory status. The patient may be in fluid overload or be running dry. Tally up your ins-and-outs to get a picture of their fluid status.
At any point if you feel the patient is decompensating, call a code. I’d rather get cancelled halfway to your room than arrive to find you doing CPR. (I get all sweaty and my hamstrings get sore. The worst.)
Whew, that was a lot. The first time this happens can feel overwhelming. Alarms are going off, people are coming and going. The patient feels terrible and scared. Family members are asking a million questions.
Your focus is the patient. Other people can deal with the circus around you. Tell family to step back or be quiet for a moment. Ask for help from your teammates. Call for resources.
You got this.
References
(1) Delle Karth, G., Geppert, A., Neunteufl, T., Priglinger, U., Haumer, M., Gschwandtner, M., Siostrzonek, P., & Heinz, G. (2001). Amiodarone versus diltiazem for rate control in critically ill patients with atrial tachyarrhythmias. Critical care medicine, 29(6), 1149–1153. https://doi.org/10.1097/00003246-200106000-00011
(2) Wikipedia contributors. (2023, February 24). Amiodarone. In Wikipedia, The Free Encyclopedia. Retrieved 07:47, April 29, 2023, from https://en.wikipedia.org/w/index.php?title=Amiodarone&oldid=1141253879
(3) Davis’s Drug Guide For Nurses. F.A. Davis Company; 2023. (mobile app)
Thank you for reading! Please subscribe and share with the buttons below. This is My Nurse Face posts bi-weekly and is completely free! I write about my experiences in the ICU and general nurse life and advice.
Follow me on Instagram to never miss a post!
If you liked this, please check out my other Substack: WritingRampant. No nursing, but occasional blood and guts. (My characters like to stab each other. Such drama queens...)
Enjoy!
Anna, RN, BSN, CCRN
