



Nurse Files: ABG Part 1
All About Blood Gases


Of all the knowledge we crammed into our brains during nursing school, the topic that caused the most consternation was interpreting arterial blood gases. We would sit tense in study groups for hours, trying to parse through the different acid-base disorders.
Compensated? Uncompensated? Mixed? Partial? Ugh.
With the grand hope to prevent further suffering by the nation’s nursing staff, here is the first in a series about the ABG and acid-base disorders.

Back to Basics
What is an ‘arterial blood gas?’ This is a blood test, usual performed by the respiratory therapist, that measures the amount of oxygen (O2) and carbon dioxide (CO2) in arterial blood. Other things are measured as well, including pH — a measure of the blood’s acidity — and the bicarbonate (HCO3) — a substance in blood that balances the acidity. (And, yes, it is the same stuff that you use when baking cookies, with a sodium attached.)
The results may have other values, depending on the machine used to run the test. You generally end up with a receipt-like slip of paper listing all these out like so many groceries:
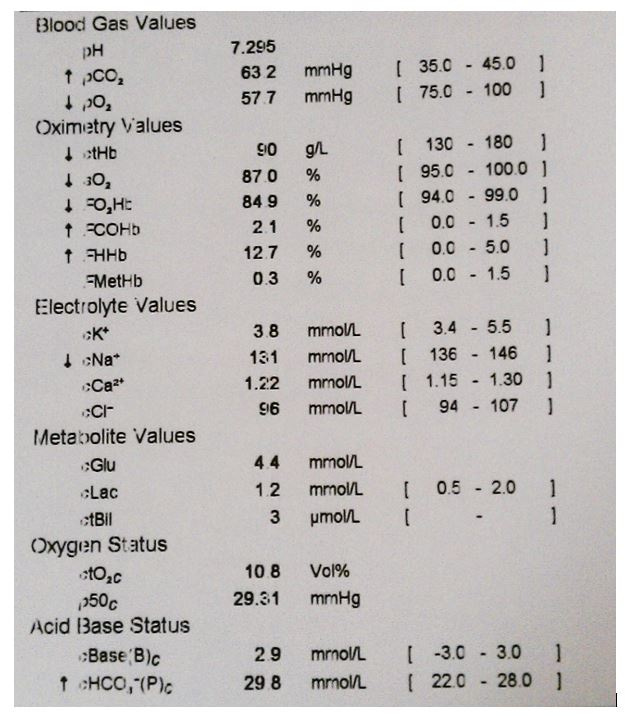
On the left you see the chemical/gas. The middle is the result, and the right is the normal range. There are even helpful little arrows to let you know which way things are out of balance.
The main values we care about when interpreting an ABG are the pH, the pCO2, the pO2, and the HCO3-.

Some Things to Remember
Blood is a liquid. It is mainly water, with a handful of blood cells, proteins, and electrolytes mixed in. This makes it a ‘solution’ and the bits it carries the ‘solutes.’ These substances, including the gases, are dispersed into the solution, much the same way CO2 is dissolved in soda.
When under a stable pressure, you cannot see the CO2 in the soda. Maybe some bubbles have aggregated, but the CO2 is dissolved to a molecular level. When you change the pressure, or open the soda bottle, the dissolved gases can release.
The same with your blood. O2 binds hemoglobin to be transported. CO2, however, has 3 different transport mechanisms:
30% is attached to hemoglobin inside red blood cells (RBC)
60% also enters the RBCs, but is turned into carbonic acid (H2CO3)
10% is dissolved just like a soda and disperses into blood as a free gas.
Now, take a look at the 2nd option. H2CO3 looks an awful like HCO3… there’s just an extra hydrogen molecule hanging about. This is because carbonic acid really likes to break apart and form H+ and HCO3-. (The pluses and minuses will be important later; ignore them for now.)
Once the RBC has made carbonic acid (H2CO3), it then breaks it apart and spits the bicarbonate (HCO3-) into solution and keeps the hydrogen (H+) attached to the hemoglobin.
Stay with me! I know I’ve started bandying about chemical formulas and you just want to know what to do if the pH is wacky. I get it. But having an understanding of where and how this stuff moves around will help you make the right clinical decisions. I promise.

Bedside Considerations
Okay, we’ve suffered through enough chemistry, what does this matter to me at bedside?
I use the ABG results to judge the body’s ability to supply oxygen to the cells and remove waste gases to the lungs. I know you can determine metabolic acid-base imbalances with an ABG, but the most common way I use them is to determine if a patient needs to be intubated or not.
This makes sense, as the metabolic acid-base compensation system is a slow process and can take a few days to kick in. In contrast, the respiratory acid-base compensation system takes minutes. If something is weird about a person’s breathing, pulling an ABG can tell us give insight to what processes are happening in the body at that moment and what we can do to fix them.
I will let this settle in your brain for now. ABG: Part 2 will cover pH and what it means for your patient.
References
Porth’s Pathophysiology: Concepts of Altered Health States (9th Edition). Grossman, S.C., Porth, C.M.
Thank you for reading! Please subscribe and share with the buttons below. This is My Nurse Face is completely free! I write about my experiences in the ICU and general nurse life and advice.
Follow me on Instagram to never miss a post!
If you liked this, please check out my other Substack: WritingRampant. No nursing, but occasional blood and guts. (My characters like to stab each other. Such drama queens...)
Enjoy!
Anna, RN, BSN, CCRN

Totally fascinating!