



Excuse me, ma'am? There's a knife in your head.

“46-year-old female, Full Code. Allergies to penicillin and amoxicillin. Came into the ED via ambulance with penetrating trauma to the skull.”
I pull up the CT images. They look something like this:

Well, Mr. ED Nurse, you are 100% correct. There is definitely some penetrating trauma to the skull. I feel, however, that starting with “there’s a knife in her head” would convey much more about the situation than what her allergies are.
Admittedly, this woman will be on antibiotics. There’s a lot of things growing on your outside that should not be on your inside, not to mention whatever nasty things are on that knife. Gross.
Report continues from there. The various things the trauma team did to save her life. How many units of blood she received. What we know about why there is a knife in this woman’s brain. ‘Tripped and fell,’ doesn’t seem realistic in this situation, but you never know.
While I prepare to receive this patient (sans knife) my mind is running through scenarios:
If she received only packed RBCs and fluids, she’ll be hypocalcemic. Hypocalcemia = impaired coagulation and cardiac compromise.
How long was she down? Hypothermia = impaired coagulation.
How much blood was lost? Blood loss + trauma = impaired coagulation.
(There’s a theme here, isn’t there?)
I am also considering intracranial pressure, cytotoxic edema, rhabdomyolysis, renal injury, other wounds, infection, toxins, not to mention the psychosocial nightmare the police and family situation will be.
I have my room set up: suction, monitor, pressure cables, iv pumps. I get elevator call (so considerate!) and the surgical team arrives. The anesthesiologist runs through their numbers and notes, my fellow RN’s help get the patient hooked up to the monitor, the RT adjusts the ventilator.
The next few hours are a blur of activity. Adjusting drips, assessing reflexes, photographing wounds. Lab draws, dressing checks, calculations. Blood pressures, urine output, heart rate, cough and gag.
The post-op CT shows the cavity where the knife had been. It is now full of fluid and air. Already the surrounding tissue is losing its differentiation; cerebral edema is setting in and will only get worse over the next two days.
Then I go eat a sandwich. It is in these quiet moments that I have time to think. Not about electrolytes and heart rhythms, but mundane things:
I wonder if she felt the knife go in? Or would unconsciousness be immediate?
How much force does it take to shove a knife through someone’s skull? Is her skull unusually thin?
Could I stab someone in the head? Or any other place? Under the right circumstances, of course…
Oop, there’s my phone alarm. Time to get back to work.
Not much changes over the rest of my shift. Little adjustments to vasopressors and sedation. Turns. Hourly urine output. I place an orogastric tube to evacuate her stomach and administer medications. I take out a gross looking field PIV.
It is always jarring, this dichotomy between the technical, inhuman part of nursing and the emotional part. There is a time and place for each, but they never sit comfortably for me.
As I assess for cortical reflexes, I am not thinking of this woman’s family. As the Intensivist fires off orders, I am not thinking of the massive brain damage this woman will have, if she survives. The police call and I have the Unit Secretary tell them to call back tomorrow, I have no new information.
Someone calls hysterical, asking about the patient. We cannot tell them anything, not even that she is admitted, to protect her and ourselves against further violence.
But the next day comes. She has survived the night. Her vital signs are not great, but not terrible. We are keeping her heavily sedated, so her brain does little more than contract her pupils when I shine a light in them. Even then, they are slow and I have to check twice.
Her identity is confirmed. The person responsible is in custody. Family can come visit. It is screaming and tears and demands to know what happened, why isn’t she waking up.
Some visitors are well dressed and white around the mouth. Others stink of tobacco and marijuana and curse every other word. This woman is the intersection of such different lives, different ways of being. The scars down her arms and legs tell me she uses IV drugs. Her medical records are sparse but paint the picture of a woman estranged from her family and fallen into destructive behavior.
And then comes the hard, soul-searching question: did she deserve this?
Can I feel compassion for this woman who made so many wrong choices? If she hadn’t been seeking out methamphetamine, she wouldn’t have been with someone who felt their differences could be solved by violence. If she had conformed to society’s standard of moral behavior, her loved ones would never have been exposed to this horror.
She’s here, in my ICU bed, using resources that I could have used for someone else. Someone who made better choices and was injured doing something worthwhile, or due to an ‘act of god.’
I don’t have the answer to this question.
I do, however, know that the Trauma Triad of Death will kill her faster than anything. That cerebral herniation will destroy any chance of her surviving, deficits or not. That infection is already setting in and her antibiotics need to be administered on time to prevent catastrophic septic shock.
So, I fix these things. I do whatever I can to keep her stable. I limit the comorbidities as best I can. I can ask myself these soul-deep questions another time. Right now, I have work to do.
The Trauma Triad of Death is an awareness of the sequalae of blood loss and how it affects the body. In short, blood loss leads to hypothermia, increased cardiac workload, and consumption of clotting factors. These in turn cause metabolic acidosis, continued blood loss, and cardiac compromise. Etc., etc., until death.
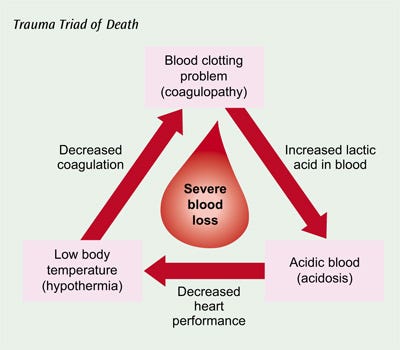
This is why trauma rooms are blazing hot and we warm blood products during a massive transfusion. It’s why temperature management is critical in trauma patients, especially those with brain injuries. It’s why you are supposed to warm a trauma patient in the field and stop the bleeding no matter what.
And it doesn’t take much to tip someone into this spiral. Children are particularly susceptible due to their larger body surface area and smaller blood volume.
Hypocalcemia is a complication of administration of blood products containing the preservative citrate, as well as the depletion of clotting factors, poor nutrition, and other disease states. Here’s a good article on it: Managing hypocalcemia in massive blood transfusion.
Moral of the story: keep your patients warm (but not too warm), replace their electrolytes and clotting factors, and reverse acidosis.
Thank you for reading! Please subscribe and share with the buttons below.
This is My Nurse Face posts weekly and is completely free! I write about my experiences in the ICU and general nurse life and advice.
If you liked this, please check out my other Substack: Writing Rampant. No nursing, but occasional blood and guts.
Enjoy!
Anna, RN, BSN, CCRN